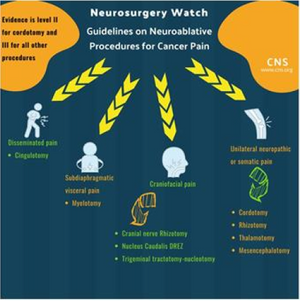
Guideline on Neuroablative Procedures for Patients with Cancer Pain

- Management of medically refractory pain in advanced cancer patients remains a significant challenge with the majority of patients experiencing pain, often unrecognized or undertreated
- Neurostimulation procedures are not appropriate for many patients and increasing doses of opioid medication can lead to opioid-induced hyperalgesia
- Neuroablative procedures have made a resurgence in an effort to fill the gaps left by other treatments
- Level II recommendation: Cordotomy should be considered for unilateral somatic pain
- Level III recommendations (categorized by type and location of pain):
- Unilateral neuropathic or somatic nociceptive pain
- Rhizotomy
- Mediodorsal and Basal Thalamotomy
- Mesencephalotomy (for dermatomes above C5)
- Craniofacial pain
- Cranial nerve Rhizotomy
- Nucleus Caudalis DREZ
- Trigeminal tractotomy-nucleotomy
- Midline subdiaphragmatic visceral pain
- Disseminated pain
- Insufficient data exits to make a recommendation regarding DREZ for unilateral body pain
Source
Source:
NEUROSURGERY